

Clinical Outcomes, Procurement Considerations & Why Your Urology Department Needs It
An evidence-based guide for urologists, department heads, and hospital procurement committees evaluating anti-retropulsion devices for ureteroscopic lithotripsy.
5–40%
370,000+
Section 01 — The Problem
Stone Migration: The Hidden Cost in Every Ureteroscopy Suite
Every urologist who has performed ureteroscopic lithotripsy knows the moment: the laser fires, the stone fragments — and a piece migrates proximally, retreating into the renal pelvis. What follows is an extended procedure, a potential second session, and a patient who is no longer stone-free at discharge.
This is not a rare event. Retrograde stone migration — or retropulsion — during ureteroscopic lithotripsy occurs in an estimated 5% to 40% of proximal and distal ureteral calculi cases. The range is wide because retropulsion is influenced by stone size, stone composition, laser settings, irrigation pressure, and the absence or presence of an anti-retropulsion barrier. Without one, every fragmentation pulse creates a hydraulic wave that propels residual concretions upward.
Departmental cost impact: Each episode of stone migration that requires a secondary flexible ureteroscopy or repeat procedure adds theatre time, anaesthesia cost, and staff utilisation — estimated at significant per-case cost overruns in high-volume urology centres.
The clinical consequences are measurable: higher residual fragment rates, more auxiliary procedures, longer hospital stays, and reduced stone-free rates at 30-day follow-up. For hospital procurement committees, this translates directly into avoidable direct cost and avoidable bed-day consumption. The solution is an anti-retropulsion device — and among available options, the Stone Cone Nitinol Retrieval Coil has the strongest published evidence base.
Section 02 — Device Overview
What Is the Stone Cone Nitinol Retrieval Coil?
The Stone Cone is a dedicated anti-retropulsion and fragment retrieval device used during ureteroscopic lithotripsy. Originally developed at Massachusetts General Hospital (Harvard Medical School) by Dr. Stephen Dretler, it was designed to solve two simultaneous problems: preventing proximal stone migration during intracorporeal lithotripsy, and enabling safe extraction of stone fragments without basket entrapment.
The device is constructed from shape-memory nitinol wire — the same material used in high-performance ureteral stents and stone baskets. When deployed, the nitinol coils expand into a tapered cone shape that occludes the ureteral lumen proximal to the target stone, acting as a physical backstop against which fragmentation can proceed unimpeded.
Stone Cone Nitinol Retrieval Coil Technical Data Sheet
| Parameter | Specification | Clinical Relevance |
|---|---|---|
| Material & Construction | ||
| Primary material | Nitinol — nickel titanium alloy | Shape-memory property ensures consistent cone expansion in vivo |
| Wire configuration | Expandable tapered coil design | Occludes ureter proximal to stone; prevents retropulsion |
| Radiopaque tip | Yes | Enables real-time fluoroscopic tracking during deployment |
| Torque device | Proximal torque handle included | Enhanced control and precise maneuvering within ureter |
| Delivery sheath | Outer sheath for controlled deployment | Straightens coil during insertion and removal for atraumatic passage |
| Dimensions & Sizing | ||
| Coil expansion diameter | > 4 mm (deployed state) | Sufficient to occlude adult ureteral lumen in proximal and distal segments |
| Safety release threshold | ~0.127 lb (approx. 57.6 g) tension | Coils >4 mm release concretions too wide for ureteral orifice — prevents entrapment |
| Minimum fragment retrieval | ≥ 1.5 mm concretions | Retrieves both whole stones and fragments post-fragmentation |
| Available sizes | Multiple sizes — supplier-specific | Size selection based on patient anatomy and ureteroscope working channel |
| Instrument Compatibility | ||
| Insertion route | Via ureteral catheter / working channel of ureteroscope | No additional access port or specialised scope required |
| Ureteroscope compatibility | Semi-rigid and flexible ureteroscopes | Validated with Karl Storz, Olympus, Wolf, and equivalent platforms |
| Lithotripsy modality | Holmium:YAG laser, EHL, pneumatic lithotripsy | Compatible with all standard intracorporeal lithotripsy modalities |
| Stone retrieval device pairing | Compatible with standard stone retrieval forceps and baskets | Cone can be used alongside retrieval tools without scope withdrawal |
| Sterilisation & Safety | ||
| Sterilisation method | ETO sterilised | Ethylene oxide — standard for nitinol devices; maintains shape-memory properties |
| Use classification | Single-use only | Reuse or resterilisation contraindicated; invalidates manufacturer liability |
| Packaging | Sterile barrier packaging, peel-open | Maintains sterility through to point of use in theatre |
| Storage conditions | Room temperature; avoid humidity and direct sunlight | Standard sterile store conditions; no refrigeration required |
| Shelf life | Typically 2–3 years from manufacture date | Confirm lot-specific expiry on packaging; relevant for par-level stock planning |
| Regulatory & Quality | ||
| Device classification | Class II medical device | Applicable under FDA, CE, and CDSCO frameworks |
| CE marking | Yes — EU MDR compliant | Request Declaration of Conformity from supplier at RFQ stage |
| FDA clearance | 510(k) cleared | Confirm current 510(k) number with supplier for procurement documentation |
| CDSCO registration (India) | Verify at RFQ | Mandatory under Medical Devices Rules 2017 for Indian hospital procurement |
| Manufacturing standard | ISO 13485 certified manufacturing | Required for NABL and JCI accredited hospital procurement |
| Clinical Use Parameters | ||
| Indicated stone location | Proximal, mid, and distal ureteral calculi | Highest retropulsion risk in proximal ureter (above sacroiliac joint) |
| Primary clinical function | Anti-retropulsion barrier + fragment retrieval | Dual function: prevents migration and enables extraction in single device |
| Deployment position | Cephalad (proximal) to the target stone | Cone opened proximal to stone before lithotripsy begins |
| Flexible scope requirement | May be eliminated | Reduces mid-case conversion from semi-rigid to flexible scope |
| Learning curve | Minimal — no additional capital equipment required | Integrates into standard ureteroscopy protocol without workflow modification |
A key safety feature: coils larger than 4 mm in diameter are engineered to release concretions that are too wide for the ureter or ureteral orifice when approximately 0.127 pounds of tension is applied — preventing ureteral entrapment, one of the most feared complications of basket-based retrieval.
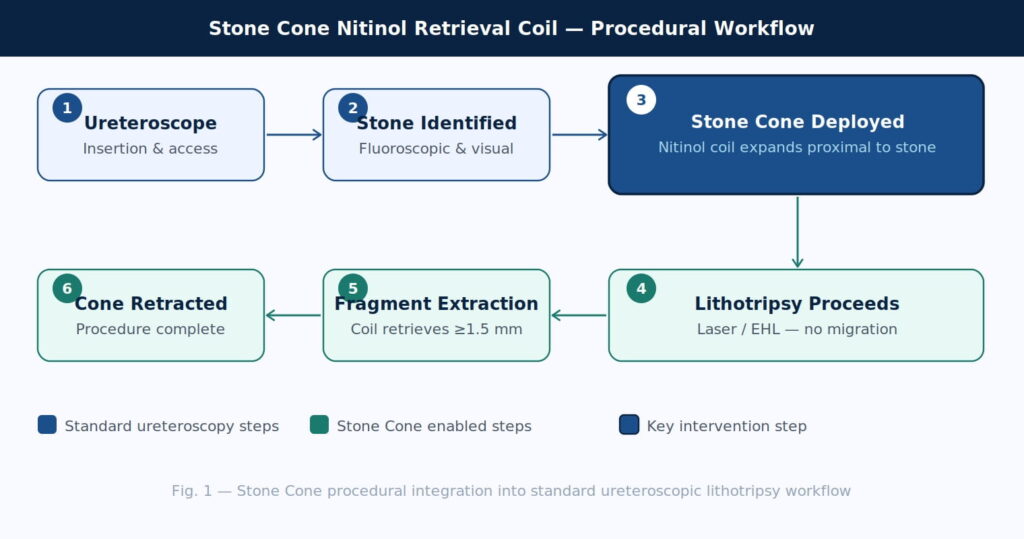
A six-step flowchart showing the procedural sequence: ureteroscope insertion, stone identification, stone cone deployment, lithotripsy, fragment extraction, and device removal.
Section 03 — Clinical Evidence
Clinical Outcomes: What the Evidence Shows
The Stone Cone has been evaluated across multiple prospective studies comparing it to conventional flat-wire stone baskets. The evidence base is consistent in its direction: the device reduces residual fragment burden, decreases the need for auxiliary procedures, and improves stone-free rates at follow-up.
Stone-free rates and auxiliary procedures
In the landmark initial clinical series (Desai et al., 2002), 50 consecutive patients with ureteral calculi were treated using the Stone Cone. The device was associated with a statistically lower incidence of significant residual fragments and fewer auxiliary procedures compared to conventional flat wire baskets — the two metrics that matter most to department heads tracking outcomes and theatre efficiency.
Fragment retrieval performance
The nitinol cone design expands to occlude the ureter proximal to the target stone and reliably extracts whole concretions and fragments of 1.5 mm and above. The tapered geometry — combined with the safety release mechanism that prevents ureteral entrapment — makes it effective across both proximal and distal ureteral locations, where the risk of retropulsion differs substantially.
Key outcome metric for procurement justification: Fewer auxiliary procedures per stone case = lower direct cost per episode, lower anaesthesia utilisation, and improved surgical throughput — all measurable at the departmental level within 6–12 months of adoption.
Anti-retropulsion in the holmium laser era
As holmium: YAG laser lithotripsy has become the standard modality for ureteral stones, anti-retropulsion devices have become proportionally more relevant. Laser pulse energy produces significant hydraulic displacement of stone fragments. Studies comparing anti-retropulsion devices including the Stone Cone with laser-only approaches have consistently demonstrated that the device increases fragmentation efficiency and reduces retropulsion events, particularly for proximal ureteral calculi above the sacroiliac joint — the highest-risk anatomical segment.
Section 04 — Device Comparison
Stone Cone vs. Conventional Flat Wire Basket: Head-to-Head
For procurement committees evaluating device options, the following clinical and operational comparison is drawn from published literature and device specifications.
| Parameter | Stone Cone Nitinol Coil | Conventional Flat Wire Basket |
|---|---|---|
| Anti-retropulsion function | Active backstop — coil occludes ureter proximal to stone | None — baskets retrieve but do not prevent migration |
| Residual fragment rate | Lower — fewer significant residual fragments at follow-up | Higher residual fragment burden reported in comparative studies |
| Auxiliary procedures required | Fewer — reduced need for repeat ureteroscopy or ESWL | Higher auxiliary procedure rate due to migration events |
| Fragment entrapment risk | Low — safety release at ~0.127 lb tension prevents basket trapping | Higher risk of basket-stone entrapment in narrow ureter |
| Minimum fragment retrieval | ≥1.5 mm concretions (whole stones and fragments) | Variable — dependent on basket wire geometry and stone shape |
| Flexible scope requirement | May be eliminated — reduces need for semi-rigid to flexible upgrade mid-case | Migration may necessitate flexible scope upgrade |
| Material | Shape-memory nitinol (consistent expansion in vivo) | Nitinol or stainless steel (varied) |
| Sterilisation | ETO sterilised, single-use | Typically single-use, ETO or gamma |
| Fluoroscopic visibility | Radiopaque tip — real-time tracking confirmed | Variable — some baskets not fully radiopaque |
Section 05 — Operational Economics
OT Economics: Translating Clinical Benefits Into Financial Metrics
For hospital administrators and purchase committees, the clinical argument for the Stone Cone must be translated into operational and financial terms. The device adds a line item cost per procedure. The case for adoption rests on demonstrating that this cost is offset — and typically more than offset — by savings elsewhere in the episode of care.
Theatre time savings
Stone migration events require the surgeon to abandon the planned semi-rigid ureteroscopy, switch to a flexible ureteroscope, and pursue fragments into the renal pelvis. This mid-case scope change adds meaningful theatre time and extends anaesthesia duration. With an anti-retropulsion device in place, this conversion is largely eliminated in straightforward cases — yielding a more predictable, bounded procedure duration and improved OT scheduling fidelity.
Reduced re-admissions and repeat procedures
Residual fragments of clinically significant size (typically >4 mm) require follow-up intervention — either a repeat ureteroscopy, extracorporeal shock wave lithotripsy (ESWL), or watchful waiting with attendant imaging. Each repeat procedure carries its own direct cost and bed-day impact. Reducing the residual fragment rate at primary procedure directly reduces this downstream burden.
Flexible scope preservation
Flexible ureteroscopes are among the most cost-intensive instruments in a urology department — acquisition cost in the range of ₹15–30 lakh per scope, with high per-use maintenance and repair expenditure. Reducing mid-case conversion from semi-rigid to flexible scope extends instrument life and reduces annual repair cost. For departments tracking per-scope utilisation, this is a measurable and reportable benefit.
Section 06 — Procurement Checklist
Procurement Considerations for Hospital Purchase Committees
The following checklist covers the key evaluation criteria for procurement teams assessing the Stone Cone Nitinol Retrieval Coil for their urology department.
- Regulatory status: Confirm CDSCO registration (India), CE marking (EU), or FDA 510(k) clearance as applicable to your procurement jurisdiction. Request documentation from the supplier at RFQ stage.
- Compatibility validation: Verify working channel diameter compatibility with your installed ureteroscope fleet (both semi-rigid and flexible). The Stone Cone is compatible with standard working channels — request a fit confirmation from the supplier with your specific scope models.
- Sterilisation and shelf life: ETO sterilised, single-use device. Confirm shelf life (typically 2–3 years) and storage requirements (room temperature, avoid humidity) for inventory planning.
- Volume-tiered pricing: Request per-unit pricing at annual commitment volumes of 100, 250, and 500 units. For high-volume centres (>300 ureteroscopies/year), bulk procurement contracts with quarterly delivery schedules reduce carrying cost.
- Trial / clinical evaluation programme: Leading suppliers offer a clinical trial allocation (typically 10–20 units) for supervised evaluation before full formulary adoption. Request this at the outset of procurement dialogue.
- In-service training: Minimal learning curve — no new capital equipment or specialised training required. Request a clinical application specialist demonstration for your urology nursing and tech team prior to first clinical use.
- Par-level stocking: Recommend maintaining a par level of 10–15% above average monthly procedural volume to avoid stockout during supplier lead times. Device is single-use; no reprocessing cost.
- Outcomes tracking for formulary renewal: Establish pre-adoption baseline metrics (stone-free rate at 30 days, auxiliary procedure rate, flexible scope conversion rate). Measure at 6 and 12 months post-adoption to support formulary renewal and budget case for continued procurement.
Section 07 — Regulatory & Standards
Regulatory Status, Compatibility & Sterilisation
The Stone Cone Nitinol Retrieval Coil is a Class II medical device under most regulatory frameworks, cleared for use in ureteroscopic procedures for the management of ureteral calculi. For procurement in the Indian market, devices must carry valid CDSCO registration under the Medical Devices Rules 2017 — verify this at the time of vendor qualification. For hospitals procuring under NABL or JCI accreditation standards, the supplier should be able to provide ISO 13485-certified manufacturing documentation.
The device is supplied sterile (ETO sterilisation), single-use only. Reuse or resterilisation is contraindicated and invalidates manufacturer liability. Ensure your department’s sterile supply protocol reflects single-use classification to prevent inadvertent reprocessing.
Compatibility with the full range of commercially available ureteroscopes — including Karl Storz, Olympus, Wolf, and Storz Flex-X series — has been validated in published clinical use. Confirm with your specific model range prior to first use.
Section 08 — Summary
Bottom Line for Your Urology Department
The Stone Cone Nitinol Retrieval Coil is the only commercially available anti-retropulsion device with a published multi-study evidence base demonstrating reduced residual fragment rates and fewer auxiliary procedures compared to conventional flat-wire baskets. It requires no capital equipment investment, no specialist training, and no modification to existing ureteroscopy protocol — it adds a single device to the procedure tray and removes the single most unpredictable variable in ureteroscopic lithotripsy: stone migration.
For high-volume urology departments, the cumulative OT time savings, flexible scope preservation benefit, and reduced re-intervention rate provide a credible financial case that exceeds device cost within the first six to twelve months of adoption at meaningful procedural volumes.
The question for your procurement committee is not whether an anti-retropulsion device is clinically justified — the evidence is unambiguous on that. The question is which device has the strongest evidence, the best safety profile, and the most favourable procurement economics. On all three counts, the Stone Cone Nitinol Retrieval Coil merits serious evaluation for formulary adoption.
Ready to Evaluate the Stone Cone for Your Department?
Request a clinical demonstration or volume pricing for your urology department. Our clinical application team can arrange an in-theatre evaluation at your facility.









Leave a Reply